If you have been researching rhinoplasty on Long Island or in Manhattan, you have probably come across the phrase preservation rhinoplasty. It comes up in before-and-after galleries, in surgeon bios, and increasingly in the questions patients bring to consultations. But what does it actually mean? And is it meaningfully different from the rhinoplasty techniques that surgeons have been using for decades?
The short answer is yes, the difference is real, and for the right patient it matters quite a lot. This article explains what preservation rhinoplasty is, how it compares to traditional structural and reduction approaches, why the technique has gained traction among facial plastic surgeons, and what it means practically for your recovery, your result, and your long-term nasal function.
A Brief History of How Rhinoplasty Got Here
Rhinoplasty has been performed for well over a century, and the dominant philosophy for most of that time was subtraction. If a patient had a bump on the bridge, the surgeon removed it. If the tip was bulky, cartilage was trimmed. The goal was a smaller, more refined nose, and for a long time smaller was considered better.
The problem with this philosophy is structural. Removing cartilage and bone from the nasal framework changes the support system of the nose. Over time, and sometimes immediately, this can lead to functional problems like breathing difficulties caused by nasal valve collapse, or aesthetic ones like the pinched, over-operated appearance that became a hallmark of rhinoplasty work from the 1980s and 1990s.
By the 2000s and 2010s, the surgical community began pushing back. Structural rhinoplasty, which focuses on rebuilding the nose with grafts rather than simply removing tissue, became the dominant approach for complex cases. It produced more durable, more natural results than pure reduction, but it is still a technique that involves significant manipulation of the existing anatomy.
Preservation rhinoplasty represents the next evolution. Rather than rebuilding what has been removed, it asks a prior question: how much do we actually need to remove in the first place? The answer, for many patients, is considerably less than traditional technique assumes.
What Traditional Rhinoplasty Involves
Traditional rhinoplasty, whether performed open or closed, typically addresses the nose by resecting, reshaping, or reconstructing its cartilage and bone structures. The most common manoeuvres include:
- Hump reduction: rasping or removing the bony and cartilaginous dorsal hump to create a straighter profile
- Osteotomies: controlled fractures of the nasal bones to narrow a wide bridge after hump removal
- Tip work: trimming, suturing, or replacing the lower lateral cartilages to refine the nasal tip
- Septal work: straightening a deviated septum, often harvesting septal cartilage for use as graft material
- Grafting: adding cartilage from the septum, ear, or rib to reconstruct areas where tissue has been removed or structural support is lacking
These are all well-established techniques with a long track record. Structural rhinoplasty in experienced hands produces good results. But by definition it involves significant manipulation of the existing nasal anatomy, which means greater disruption to tissue planes, more post-operative swelling, a longer period of bruising, and more variables that must be managed through the healing process.
There is also a structural consequence to consider. Every piece of cartilage removed is structural support that no longer exists. In aggressive reduction cases, this can lead to weakening of the nasal framework over the years following surgery, producing the collapse and breathing difficulties that bring patients to revision surgeons.
What Preservation Rhinoplasty Is and How It Differs
Preservation rhinoplasty takes a fundamentally different approach to the same problems. Rather than removing the dorsal hump, the surgeon displaces it, lowering the entire nasal roof as a unit while keeping the native cartilage and ligament connections intact. Rather than fracturing the nasal bones to close an open roof, the preservation technique avoids creating the open roof in the first place.
The central concept is that the nose has an existing architecture that, where possible, should be respected rather than dismantled. The surgeon's job is to work within that architecture, repositioning, refining, and reshaping, rather than reducing it to component parts and rebuilding from scratch.
In practical terms this means:
- Less resection of cartilage and bone, so the structural support of the nose is maintained
- Fewer or no osteotomies in many cases, reducing trauma to the nasal bones and surrounding tissue
- Maintained ligament attachments, which contributes to more natural movement and appearance post-operatively
- Reduced need for cartilage grafting, because less has been removed and less reconstruction is therefore required
- Lower risk of long-term structural weakening, because the native framework remains largely intact
Dr. Doshi's approach to preservation rhinoplasty also incorporates PISO, piezoelectric ultrasonic bone work, which replaces traditional rasping and osteotomies with ultrasonic instrumentation. This allows for more precise bone work with significantly less trauma to the surrounding soft tissue, reducing post-operative bruising and swelling compared to conventional methods. It is one of a small number of additional refinements that separates preservation rhinoplasty as Dr. Doshi performs it from earlier iterations of the technique.
The Role of the Open Roof and Why It Matters
One of the key technical differences between preservation and traditional rhinoplasty is how the open roof problem is handled, and this is worth explaining in plain terms because it illustrates why preservation produces less swelling and a faster recovery.
In traditional hump reduction, the surgeon removes the cartilaginous and bony hump by rasping it down or excising it directly. This creates what surgeons call an open roof: a gap in the nasal bone structure where the hump used to be. To close this gap and prevent a flat or boxy dorsum, osteotomies are then performed, fracturing the nasal bones inward to bring them together.
Osteotomies are effective, but they are also the primary cause of the significant bruising and swelling associated with rhinoplasty recovery. Fracturing the nasal bones produces trauma to the surrounding tissue that takes two to three weeks to visibly resolve, and longer to fully settle internally.
Preservation rhinoplasty avoids this sequence entirely. By using a let-down or push-down technique to lower the nasal dorsum as a unit rather than removing it, the open roof is never created. Without an open roof, osteotomies are often unnecessary. Without osteotomies, the most traumatic component of conventional rhinoplasty is eliminated, and recovery is correspondingly faster and less disruptive.
Who Is a Good Candidate for Preservation Rhinoplasty?
Preservation rhinoplasty is not a universal solution. It is most appropriate for patients who meet the following criteria:
- Patients with a dorsal hump they want reduced. This is the primary indication, and the technique was largely developed to address exactly this concern in a less destructive way.
- Patients with intact baseline nasal structure. The preservation approach relies on working with existing anatomy, so a functional native framework needs to be present.
- Patients undergoing primary rhinoplasty. Revision cases, where prior surgery has already altered the anatomy and produced scar tissue, typically require structural reconstruction rather than preservation.
- Patients whose primary concern is the bridge rather than the tip. Significant tip work, particularly tip projection or rotation, sometimes requires techniques that are not strictly preservation-based.
- Patients who want a natural-looking result. Because the native architecture is maintained, results tend to look and move more naturally than heavily reconstructed noses.
For patients who need significant tip reconstruction, complex asymmetry correction, saddle nose repair, or revision after a prior procedure, traditional structural techniques remain more appropriate. The right approach depends entirely on the individual's anatomy and goals, which is why an in-person physical examination is a non-negotiable part of rhinoplasty planning.
For patients considering revision rhinoplasty specifically, Dr. Doshi's revision rhinoplasty page covers the additional complexity of operating on a previously altered nose and what that means for technique selection.
How Recovery Compares Between the Two Approaches
One of the most significant practical differences between preservation and traditional rhinoplasty is the recovery experience. Because the preservation approach minimises disruption to the nasal bone and cartilage framework, patients typically experience:
- Less bruising and periorbital swelling. The black eyes commonly associated with rhinoplasty are caused largely by osteotomies. Fewer or no osteotomies means significantly less discolouration in the first one to two weeks.
- Faster resolution of swelling. With less tissue trauma, the inflammatory response is reduced and swelling subsides more quickly in the early post-operative period.
- Earlier visibility of results. Patients can see a clearer picture of their outcome sooner, because residual swelling from the procedure itself is less prolonged.
- Comparable final timeline. The deep structural swelling that determines the true final result still takes twelve months to fully resolve, as it does with any rhinoplasty.
Most patients, regardless of technique, wear a nasal splint for approximately one week and can return to desk work within ten to fourteen days. Strenuous exercise is avoided for four to six weeks. The key difference is in the social recovery window, the period when bruising and visible swelling make it obvious that surgery has been performed. In traditional rhinoplasty this is typically two to three weeks. In preservation rhinoplasty with PISO bone work, many patients are presentable within ten days to two weeks.
Dr. Doshi provides detailed pre-operative and post-operative guidance to all rhinoplasty patients. His rhinoplasty pre-operative instructions and post-operative recovery tips cover what to do in the weeks before and after surgery to optimise the result.
Dr. Doshi's Approach: Breathing First, Aesthetics Second
One of the defining features of Dr. Doshi's rhinoplasty philosophy, and the reason preservation technique fits naturally within his practice, is the sequencing of priorities. He approaches every rhinoplasty with breathing function as the first consideration, not an afterthought.
The nose exists to breathe. Its functional role as part of the upper airway is primary. Its aesthetic role, while genuinely important, is secondary to that function. In traditional reductive rhinoplasty, aggressive removal of cartilage and bone can compromise the nasal valve, the narrowest part of the nasal airway, leading to breathing difficulties that persist long after the cosmetic result has settled. Some patients do not notice the functional compromise until years later, when the weakened framework begins to collapse under the pressures of normal breathing.
Preservation rhinoplasty, by maintaining the structural support of the nose rather than removing it, is inherently more protective of nasal function. This is not a coincidence. The technique was developed partly in response to the functional consequences of over-aggressive reduction, and its principles are grounded in a respect for the airway alongside the aesthetic outcome.
Dr. Doshi trained in otolaryngology, head and neck surgery, before specialising in facial plastics. His foundation is in the surgical anatomy of the airway as much as the aesthetics of the nose. That background is directly relevant to how he approaches rhinoplasty planning: not just what the nose should look like, but how it should function for the next thirty or forty years. A rhinoplasty that produces a beautiful result at two years but compromised breathing at ten years is not, in Dr. Doshi's view, a successful outcome.
For patients who have existing breathing concerns alongside aesthetic goals, non-surgical rhinoplasty can address some contour concerns without surgery, while surgical approaches address both function and form simultaneously. Dr. Doshi discusses both pathways honestly at consultation.
Preservation Rhinoplasty and Ethnic Identity
For patients from South Asian, Middle Eastern, East Asian, African American, or Latin American backgrounds, or any heritage where the nose carries cultural and personal significance, preservation rhinoplasty has particular relevance.
The traditional model of rhinoplasty, built around a Caucasian aesthetic ideal and executed through reduction, left a long record of results that patients of diverse backgrounds describe as looking wrong, inconsistent with their face, their family, their identity. The over-reduced nose, the scooped bridge, the pinched tip: these are results that subtraction-first technique produces when applied without cultural sensitivity, and without a genuine understanding of what the patient actually wanted.
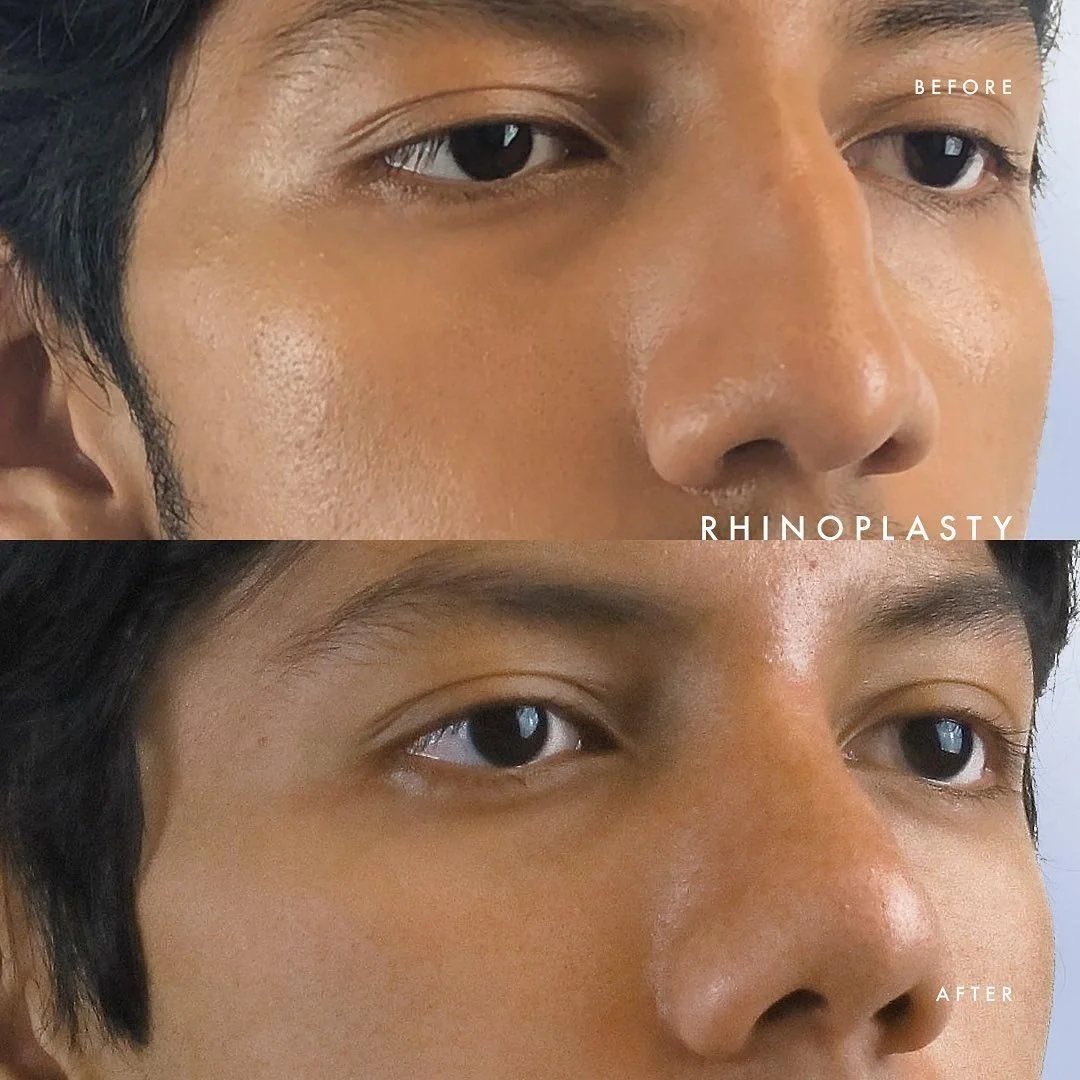
Preservation technique, because it works with the existing architecture rather than replacing it, is structurally aligned with the goals of a culturally sensitive approach to rhinoplasty: to refine without erasing. When the nasal dorsum is displaced rather than removed, the underlying shape remains the patient's own. What changes is the proportional relationship, not the fundamental character of the nose.
Dr. Doshi treats the nose as what he describes as the heirloom of the face, something inherited, something specific to that person. The goal of the surgery is to address what the patient wants to address, while preserving the characteristics that make the nose theirs. For patients of South Asian, Middle Eastern, or East Asian backgrounds in particular, this philosophy translates directly into a consultation process that begins with what the patient wants to keep, not just what they want to change.
Dr. Doshi performs ethnic rhinoplasty on Long Island for patients of all backgrounds, with a surgical plan built specifically around each individual's anatomy, heritage, and stated goals.
The Revision Rhinoplasty Problem and Why Technique Matters
One of the strongest arguments for preservation over aggressive reduction is what happens when things go wrong or when the patient is not satisfied. Revision rhinoplasty is significantly more complex than primary rhinoplasty, and the more tissue that was removed in the original procedure, the harder the revision becomes.
A nose that has been aggressively reduced has less structural material to work with. Cartilage that was removed cannot be put back. The surgeon performing a revision must typically harvest replacement cartilage from the ear or rib, adding complexity, additional recovery, and donor site considerations to an already challenging procedure.
Preservation rhinoplasty, by leaving the native architecture largely intact, produces a nose that is in a substantially better position if revision is ever needed. There is more tissue to work with, fewer compromised tissue planes, and a more predictable structural foundation.
Dr. Doshi is candid about revision complexity with all his patients. He performs revisions on patients from other surgeons regularly, and he approaches each case with a clear-eyed assessment of what the original procedure left behind and what is realistically achievable given that starting point.
For patients who have already had a rhinoplasty elsewhere and are unhappy with the result, Dr. Doshi's revision rhinoplasty practice on Long Island covers what to expect and how the approach differs for secondary cases.
Female Rhinoplasty and Preservation Technique
For female patients, the aesthetic goals of rhinoplasty often centre on refinement rather than dramatic reduction. The ideal result is typically a nose that looks naturally feminine, proportional to the patient's face, and consistent with their overall features rather than one that reads as surgically altered.
These goals align well with the preservation philosophy. By working with the existing structure rather than removing it, preservation rhinoplasty tends to produce results with softer edges, more natural tip movement, and a less operated appearance than aggressive reduction. The maintained ligament attachments mean the nose moves more naturally with facial expression, which contributes significantly to how natural the result looks in animation, not just in static photographs.
Dr. Doshi's approach to female rhinoplasty on Long Island is built around these principles: preservation of natural movement, refinement of specific concerns, and results that look like a better version of the patient's existing nose rather than a replacement for it.
Questions to Ask Your Surgeon Before Rhinoplasty
If you are evaluating rhinoplasty surgeons on Long Island or in Manhattan, the following questions will help you understand their approach and assess whether they have genuine experience with preservation technique:
- Do you perform preservation rhinoplasty, and if so, would you consider me a candidate based on my anatomy?
- What is your approach to nasal function, and will you assess my breathing as part of the surgical plan?
- How many rhinoplasty procedures have you performed, and what percentage used a preservation approach versus traditional structural technique?
- Do you use PISO or piezoelectric ultrasonic instrumentation for bone work, and what difference does that make for recovery?
- Can I see before-and-after photographs of patients with a similar anatomy, heritage, or presenting concern to mine?
- If I needed a revision in the future, how would the approach I have now affect those options?
A surgeon with genuine experience in preservation rhinoplasty will be able to answer these questions specifically, explaining not just whether they offer the technique but why your anatomy does or does not make you a good candidate for it.
Scheduling a Consultation with Dr. Doshi
Dr. Hardik Doshi is a double board-certified facial plastic and reconstructive surgeon with offices in Long Beach, Huntington, and Manhattan. He performs preservation rhinoplasty as his primary approach for primary rhinoplasty cases where anatomy and goals support it, and uses PISO ultrasonic technique for bone work to minimise trauma and recovery time.
His double board certification covers both the American Board of Facial Plastic and Reconstructive Surgery and the American Board of Otolaryngology Head and Neck Surgery. That dual certification means his training encompasses the functional anatomy of the nasal airway alongside the aesthetic goals of facial plastic surgery, which is directly relevant to how he approaches rhinoplasty planning.